COMING SOON
NOVEMBER 2018
(date to be announced)
New Jersey

HANDS-ON SURGERY & PROSTHETICS PROGRAM
Available ONLY to current Misch program attendees & former Misch graduates*
Learn & participate in surgical & prosthetic procedures on patients*
SURGICAL PROCEDURES: Difficult extractions, socket grafting, membrane augmentation, implant placement, sinus augmentations – transcrestal & lateral wall
PROSTHETIC PROCEDURES: Single, multiple crowns , full -arch zirconia prosthesis digital impressions, RFA, cement & screw-retained prostheses
*Restrictions: Valid license from any state, bring your own patients or patients provided by the Institute
#1: CBCT PATHOLOGY
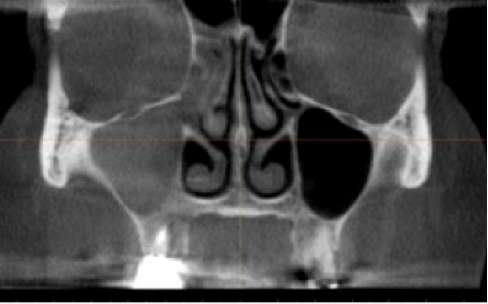
Upon CBCT evaluation of a patient, you notice the following incidental finding in the right maxillary sinus.
a. What is the differential diagnosis for this finding?
b. You refer the patient to an ENT physician for evaluation and treatment. How would you describe this condition radiographically in your referral letter?

#2: CBCT ANATOMY
In this coronal CBCT image for evaluation of posterior maxilla (for evaluation of sinus grafting), what three anatomic variants are present which may predispose the patient to mucociliary clearance complications post-operatively?
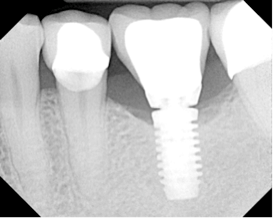
#3: Prosthetics
One of the most common post-operative complications which occurs after prosthesis completion is abutment screw loosening. Various studies have reported a prevalence to be approximately 5 – 60% of cases. A common etiologic factor contributing to screw loosening is inadequate preload, which may be due to the “settling effect.” What is the settling effect and how can it be prevented?
# 4: Legal – Medical
FRANK R. DELUCA DMD, J
Malpractice Attorney, Ft. Lauderdale, FL
deluca1958@yahoo.com
What does a implant practitioner do when he/she recommends a CBCT for a patient and the patient refuses and the legal ramifications?

Medical Emergencies Implant Patients
July 12, 2018
Orlando, FL

Surgical Program Session 4
July 13-14, 2018
Orlando, FL

Prosthetic/Surgical Program
September 14, 2018
Las Vegas, NV
CE ANSWERS:
Question #1: CBCT Pathology
#1a
- Odontogenic Rhinosinusitis
- Acute Rhinosinusitis
- Allergic Rhinosinusitis
- Primary Mucocele
- Fungal Rhinosinusitis
- Neoplasm
#1b
- Non-Patent Maxillary Ostium and Osteomeatal Complex
- Completely Opacified Maxillary Sinus and Ethmoid
Question #2: CBCT Anatomy
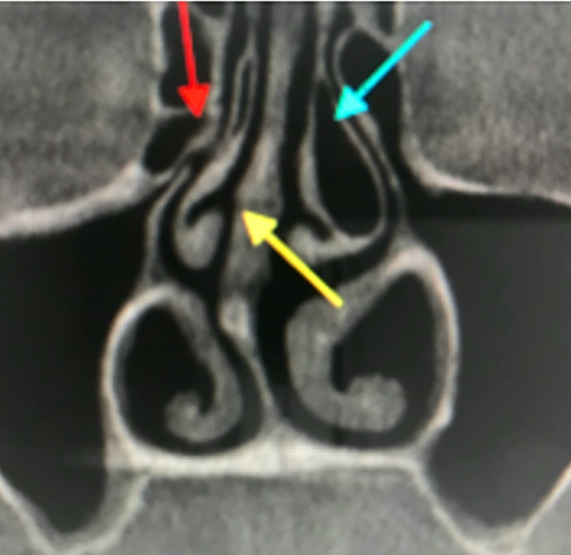
- Concha Bullosa – aerated middle turbinate, deflecting the unicinate process laterally, closing off the ostium (Prevalence = 34 %)
- Deviated Septum – deviation of the septum to one side, resulting in compressing middle turbinate laterally, closing off the ostium (Prevalence = 80 %)
- Paradoxical Middle Turbinate – backwards middle turbinate, projects laterally, blocking middle meatus and blocking the ostium (Prevalence = 26 %)
Question #3: Prosthetics
Once an abutment screw is torqued to the manufacturers specifications, there is an immediate loss of the preload (torque). This is termed “settling effect” and can be mitigated by using the following technique:
- Torque abutment screw to the appropriate manufacturer specifications.
- Wait 10 minutes and re-torque to those same specifications.
This technique will increase the torque back to the original preload, thereby decreasing the possibility of screw loosening.
Question #4: Medical – Legal
Usually, the refusal of a CBCT is the result of either radiation exposure or cost.
- Radiation exposure. The dosage of radiation from a typical CBCT is minimal.We are exposed to normal background radiation exists in the environment every day. The amount of radiation from a typical CBCT is the equivalent of normal life expose for approximately a two week period.Therefore, the patient should be educated on minimal amount of exposure from a CBCT.
- Cost. The easiest way to deal with the cost issue is to build the expense into the cost of the implant(s). If this is not feasible, for example for insurance reasons, then the patient needs to be educated on the significant advantages of a CBCT as compared to 2d radiography. Such education should include a demonstration of CBCT and its advantages over standard dental radiography. Our experience has shown that most patients are taken to technology and would like to see the best and most up to date methods used to treat them. The legal community attempted to deal with such patients by the use of a concept known as “informed refusal”. Informed refusal is where a patient, based on an complete understanding of the facts, implications and risks of not following a recommended course of treatment, declines a particular procedure. This legal concept is an offshoot of the “informed consent” process. In sum, a patient has a right to consent to treatment, as well as to refuse treatment with the caveat that they must be full informed of the consequences. Lawyers have devised an “informed refusal” form. Such language and execution by the patient is not however a panacea. It is not a get out of jail free card. Such forms should in this writers opinion be used with extreme caution. Always remember that ultimately you are the trained educated practitioner. You are charged with the ethical duty to treat patients appropriately. Patients cannot consent to negligent care .If it is against your best judgment to do the case without a CBCT, then do not proceed. In the long run you will save yourself a lot of headaches and time.